
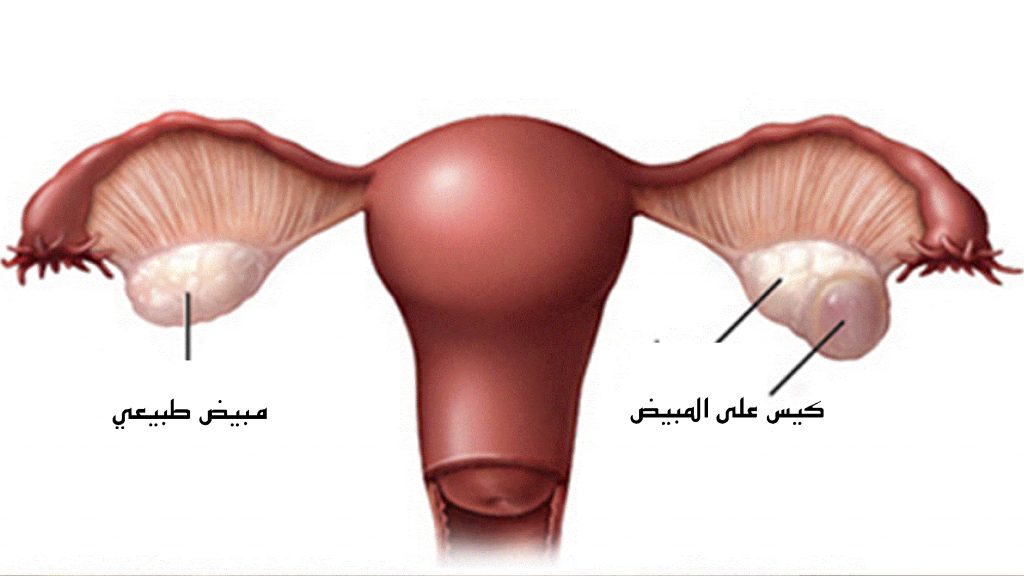
Ovarian Cysts
Ovarian cysts are sacs filled with fluids on or in the ovary.
Size: from 1 cm to more than 10 cm.
Causes:
In Premenopausal women:
– Functional:
a. Follicular: when the follicle does not rupture to release the egg.
b. Corpus luteum cyst: after the follicle releases the egg, estrogen and progestin start to produce for pregnancy, but sometimes the fluids accumulates inside the follicle resulting in growing a cyst.
– Dermoid cysts, contain tissues such as hair, skin or teeth.
– Endometriosis.
– Severe pelvic infection.
– Non-cancerous growths.
– Cancer: rare, less than 1%.
– PCO, when the ovary is enlarged, and multiple small cysts.
In Postmenopausal women:
– Fluid collection in the ovary.
– Non-cancerous growths.
– Cancer.
Risk factors:
– Previous ovarian cysts.
– Hormonal imbalance.
Cancer or not?
Ovarian cancer is not the most cause of cysts.
The following characteristics are considered:
– Family history of ovarian cancer.
– Previous history of breast or gastrointestinal cancer.
– Complex cyst such as with solid areas.
– Fluid collection found in the pelvis or abdomen.
Still these characteristics are not enough and further testing is recommended.
Symptoms:
Ovarian cysts can be asymptomatic.
If symptomatic, the symptoms include:
1. Pelvic pain or pressure, on the side of the cyst.
2. Pain during intercourse.
3. Frequent urge for urination.
4. Bloating or difficulties in emptying the bowel.
5. Feeling full quickly.
Complications:
1. Ovarian torsion: Cysts can enlarge and cause the ovary to move/twist. This causes severe pain and vomiting.
2. Rupture, causing severe pain and internal bleeding.
3. Possibility of malignancy.
Diagnosis:
– Pelvic exam.
– Transvaginal ultrasound.
– CT scan or MRI might be used.
– Blood tests include:
a. Pregnancy test for premenopausal women.
b. CA-125 blood test, recommended with postmenopausal women, very large cyst or suspicious for cancer.
Treatment:
Cysts usually do not need treatment.
They often resolve on their own within 1 – 2 months in premenopausal women.
Treatment approaches:
1. Watchful waiting: making sure cysts do not enlarge or resolve in their own:
A. Premenopausal women:
– Symptoms monitoring .
– Repeating pelvic ultrasound after 6 – 8 weeks.
– Birth control pill might be advised to help prevent developing new cysts.
B. Postmenopausal women:
– If the cyst does not appear to be cancerous (results of ultrasound and CA-125).
– Pelvic ultrasound and CA-125 tests need to be done every 3 – 6 months for one year, or until the cyst resolves.
2. Surgery:
Surgical treatment is recommended when:
– Cyst is caused by endometriosis.
– Cyst is causing persistent pain or pressure.
– Possibility of rupture or torsion.
– Large cysts, >5 – 10 cm.
– Cyst does not resolve after several ultrasounds.
– Suspicion for cancer.
– Present in both ovaries.
– Before puberty.
– After menopause.
Surgery is done by laparoscopy, or by laparotomy if the cyst is large or there is suspicion for cancer.
After the surgery with premenopausal women, taking birth control pills or other form of hormonal birth control may help to prevent cysts from developing.
Cases where ovaries might be removed:
– Suspicion for cancer.
– Cyst completely replaced the entire ovary.
– Blood supply to the ovary has cut off because of the cyst.

